

2011 CITY OF ST. LOUIS
WRONGFUL DEATH MEDICAL MALPRACTICE
NEGLEGENT FAILURE TO PERFORM CESARIAN SECTION
Parties: Young unmarried mother and father of decedent, ob-gyn physician and hospital
Type of Claim: We concluded a suit against a physician and hospital for wrongful death of full term fetus that was still born. It was alleged that the physician waited too long to call for an emergency caesarean section or c-section. The fetal heart monitor tapes showed fetal tachycardia and bradycardia for durations that made the tracings non-reassuring. The situation worsened so that other patterns emerged including: saltatory variability; variable decelerations associated with a non-reassuring pattern; late decelerations without preserved beat to beat variability; persistent late decelerations with loss of beat to beat variability; non-reassuring variable decelerations associated with loss of beat to beat variability; prolonged severe bradycardia; and sinusoidal pattern.
The hospital failed to have an available operating room and failed to open an operating room in a timely fashion.
There is evidence of a standard of 30 minutes to perform a cesarian section upon the call of emergency. The parties agreed to contribute to a confidential settlement. The case settled during a recess of the physician’s deposition.
Damages: death of fetus and loss of society, services and relationship opportunities with deceased son.
Comments: Settlement amount confidential. A full understanding of the standards applicable to ob-gyn physicians and maternity hospitals is necessary to properly pursue these devastating cases. All obstetrical hospitals must be able to start emergency C-sections within 30 minutes. The Guidelines for Perinatal Care state in relevant part:
… [T]he consensus has been that hospitals should have the capacity of beginning a Cesarean delivery within 30 minutes of the decision to operate.

c-section
ACOG Committee Opinion #256 states in pertinent part that “for any hospital providing obstetric care,” there should be:
Availability of anesthesia and surgical personnel to permit the start of cesarean delivery within 30 minutes of the decision to perform the procedure.
The standard of care, however, does not allow caregivers to wait 30 minutes to commence a stat C-section, if it can be done faster. Rather, caregivers are required to perform stat C-sections ” as rapidly as possible.”‘ (Of course, ” purposeful delays of any time period would be inappropriate .”‘) Thus, if the stat C-section in a given case can be performed in, e.g., eight minutes, it is inappropriate to delay commencing the surgery for the remaining 22 minutes.
The American Academy of Pediatrics (AAP) and the American College of Obstetricians and Gynecologists (ACOG), two of the main accrediting organisations in the US, recommend 30 minutes from decision‐to‐incision for emergency caesarean delivery. This standard is in the American Academy of Pediatrics, The American College of Obstetricians and Gynecologists Guidelines for perinatal care. Fifth edition. Washington, (DC): American Academy of Pediatrics [and] The American College of Obstetricians and Gynecologists, 2002. 147. See our blog on Emergency Caesarean Sections.
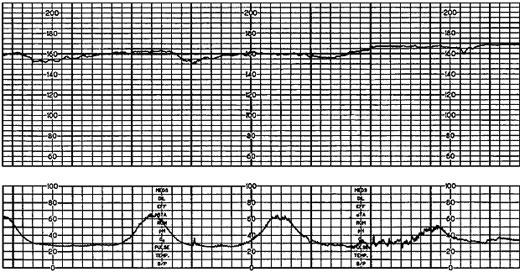
Fetal heart tracing with loss of beat to beat variability.
Recent Comments